Introduction and Intent – January 15th 2026
I am a full-time faculty member of Medical Laboratory Assistant (MLA) program, bringing a strong academic and clinical background to my teaching practice. I hold an Honours degree in Applied Biomolecular Science and completed my Medical Laboratory Technologist (MLT) program at St. Lawrence College.
Prior to joining Confederation College, I worked as a Medical Laboratory Technologist at Thunder Bay Regional Health Sciences Centre for 10 years, gaining experience across a variety of specialty areas. Teaching has long been a passion of mine, and I have previously taught within the MLA program, including delivering compressed laboratory sessions at the Thunder Bay campus on weekends—an experience I greatly enjoyed.
I transitioned into full-time faculty because of my genuine love for teaching and my commitment to supporting students as they progress toward successful careers in healthcare. I am excited to be part of the Confederation College team and to contribute to future efforts to bring the MLT program to the college, helping address the ongoing shortage of medical laboratory professionals in Thunder Bay and surrounding communities.
Professionalism and Regulation – January 18th 2026
As a Medical Laboratory Technologist (MLT) I am regulated by the College of Medical Laboratory Technologist of Ontario (CMLTO). This is a yearly registration and requires a fee to be paid. The CMLTO regulates all MLTs and acts as the governing body to set the standards for practising MLT. They also investigate complaints about the MLT’s professional conduct. Each year we are required to maintain competency through continuing educations. We set goals each year that align with the vision and values of the CMLTO. We must complete our goals for the year and submit them to the CMLTO through our portal by the end of March. We are expected to maintain an active portfolio and document all additional training and education that are in support of our goals. The CMLTO which select at random, MLT’s to audit through questionnaires, proof of insurance or submission of a completed portfolio.
As part of the Equal Accreditation and Accreditation Canada of our MLA program at the College, I must also belong to the Medical Laboratory Professional’s Association of Ontario (MLPAO). The MLPAO is a non-profit health professional organization who represents the interest of the medical laboratory profession in Ontario. They work with the government, regulatory bodies, educational institution such as our college, other health care professions and stakeholders. They is also another certification body for Medical Laboratory Assistants who work in Ontario exclusively. As part of their membership, they do offer free continuing education courses as well as liability insurance for practising medical laboratory professionals.
Medical laboratory professionals work with other medical professions. We work closely with nurse (RN and RPN), as they are often the ones placing the orders for testing for the doctors. In acute care facilities, we report critical reports to the nurse of the patient they are treated. We often work with a variety of doctors, from general practitioners to pathologist and coroners as well as specialists such as hematologists, surgeons and intensivist. We also work with the community in outpatient laboratories to provide laboratory test of all specimens, specimen collection and procurement and ECGS.
Professionalism in the Age of Social Media – January 20th 2026
What is an appropriate social media presence?
An appropriate social media presence for someone life me who is an MLT, professor at a college, parent, and vice chair of a board for a childcare center should represent an individual with respect, professionalism and good judgment. I believe that my online content should demonstrate ethical and professional standards by respecting confidentiality, communicating respectfully, and avoiding posts that may undermine trust in my profession or the community. It is imperative to have clear boundaries with my students and to keep personal and professional accounts separate. (Facebook and LinkedIn). I maintain privacy settings and I keep my content lighthearted and generic. Having a thoughtful and selective social media presence helps maintain trust with my community while still allowing for some personal expression.
How does your response consider professional ethical standards?
The Canadian Society for Medical Laboratory Science (CSMLS) Code of Ethics sets the minimum standards for ethical behaviour that is expected of its members. The code is not meant to stand alone and should be used together with other professional guidelines, including standards of practice and codes of professional conduct. When more than one policy applies to a situation, the policy with the strictest requirements should be followed. Ethical principles in the code are connected, as most ethical issues in healthcare are complex and cannot be addressed separately. To support ethical decision-making, CSMLS encourages ongoing education in ethics and recommends seeking guidance from regulatory bodies or other qualified professionals when ethical concerns arise (Canadian Society for Medical Laboratory Science 2020). This code of ethics was developed by the CSMLS and its members to uphold a their vision through specific set of principles of ethical conduct. These principles focus on 5 key areas which include safe practices, confidentiality, professional development, accountability and behaviours and attitude. Their goal is to ensure all patients are to treated equality and that quality of care is a right and not a choice.
The College of Medical Laboratory Technologist of Ontario (CMLTO) the regulatory body of MLT’s provide additional guidance by outlining expectations for both professional and personal conduct across all areas of practice. It establishes the minimum standards of ethical behaviour required of all MLTs and applies at all times. Central to the Code is the obligation to patients, which requires MLTs to place patient interests above their own by practicing competently, honestly, and with respect for patient autonomy, informed consent, and confidentiality. The Code also emphasizes obligations to the public by encouraging respectful, accessible, and collaborative interactions while promoting understanding of the profession. In addition, MLTs have obligations to the profession and regulatory bodies through lifelong learning, ethical conduct, conflict-of-interest management, and compliance with laws, standards, and guidelines. Finally, the Code highlights obligations to oneself by stressing personal accountability, practicing within one’s scope of competence, recognizing limitations, and continuously developing knowledge and skills to ensure safe and high-quality patient care (College of Medical Laboratory Technologist of Ontario 2017).
As a professional are you obligated to speak in public?
As a professional, I am not required to speak publicly beyond what my role involves. Teaching students and communicating with other professionals, including faculty from other disciplines and members of the leadership teams are considered parts of my position. My responsibility is to communicate respectfully, accurately, and within my scope of practice.
References
College of Medical Laboratory Technologist of Ontario. (2017). Code of Ethics for Medical Laboratory Technologists.
Canadian Society for Medical Laboratory Science. (2020). CSMLS Code of Ethics Guidance Document.
What is Health – February 10th 2026
Anyone entering a health care profession will find it helpful to understand the concepts of health and wellness. It is important to recognize what makes people ill and how preventable poor health can be. Many questions arise when we think about health: Was it preventable? Do life circumstances play a role in health? How does mental health affect physical health? How do individuals view their own health in comparison to their peers?
The answers to these questions vary depending on the individual, population group, life circumstances, and the social determinants of health. While some medical conditions are preventable, health promotion initiatives have increasingly focused on reducing risky behaviours and improving lifestyle choices in primary care. This raises an important question: why do individuals continue to engage in health-risk behaviours that may lead to illness, disability, or even death?
Many people take “good health” for granted until they are faced with illness or injury. Some individuals engage in “risky” behaviours such as smoking or drug use that place their health at risk and may find it difficult to stop, even when aware of the consequences. Others may believe they are immune to illness or serious health outcomes. Additionally, some people experience circumstances beyond their control, such as economic hardship, marginalization, or mental health challenges, all of which can negatively affect overall health.
In 1986, the World Health Organization (WHO) expanded its definition of health to include “the ability to identify and realize aspirations, to satisfy needs, and to change or cope with the environment.” Health was described as a resource for everyday life rather than the objective of living, emphasizing social and personal resources alongside physical capabilities. This revised definition moved beyond the original description of health as “a state of complete physical, mental, and social well-being.” The term “complete” was unrealistic and difficult to define, as many individuals live long, fulfilling lives while managing chronic diseases such as diabetes or cancer, or while living with physical or intellectual disabilities. For many, these conditions become their new “normal,” and they still consider themselves healthy.
This expanded definition of health also allows for a more holistic view, incorporating spiritual and cultural perspectives often emphasized in different cultures. As a result, the meanings of health, wellness, disease, illness, and disability continue to evolve and differ among individuals.
There are several health models used in health care delivery, including the medical model, holistic model, and wellness model. The medical model focuses primarily on the absence of disease and follows a structured process involving patient history and diagnostic testing leading to diagnosis, and treatment. The holistic model considers all aspects of an individual’s well-being and focuses on strengths and positive health outcomes rather than solely on illness. The wellness model combines elements of both approaches and views health as a dynamic, ongoing process prioritizing growth and movement towards improved well-being. This model is commonly used in today’s health care system.
It is also important to recognize the Indigenous Wholistic Theory, which aligns with holistic principles but extends beyond the individual to include the mental, physical, cultural, and spiritual well-being of not only the individual but the entire community. This perspective highlights the importance of connection, balance, and collective health.
Ultimately, health cannot be defined by a single standard or experience. It is shaped by personal choices, social environments, cultural beliefs, and circumstances that may be beyond an individual’s control. Understanding health as a dynamic and evolving concept allows health care professionals to move beyond simply treating disease and instead support individuals and communities in meaningful and respectful ways. As perspectives on health continue to change, it invites us to reflect not only on how we define health for others, but also how we understand and value health in our own lives.
References
Thompson, V. D. (2024). Health and health care delivery in Canada (4th ed.). Elsevier.
World Health Organization. (1948). Preamble to the Constitution of the World Health Organization as adopted by the International Health Conference. World Health Organization.
World Health Organization. (1986). Health promotion: Concepts and principles in action – A policy framework. WHO Regional Office for Europe.
Understanding the Social Determinants of Health in Canada – February 17th 2026
In Canada, social, economic, and environmental factors significantly impact individual and community health. People’s experiences with the health care system are influenced by ethnicity, culture, language, sex, gender, and prior interactions with health services (Government of Canada, 2024). These factors can affect access to care, quality of treatment received, and overall health outcomes.
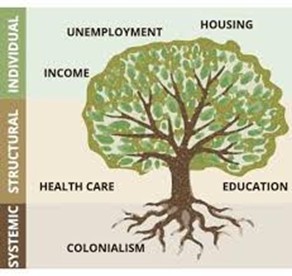
Health Canada and the Public Health Agency of Canada (PHAC) identify key social determinants of health, known as the conditions in which individuals are born, grow, live, work, and age (Public Health Agency of Canada [PHAC], 2024). These determinants are interconnected and influence well-being and overall health.
Income and Social Status. Income is one of the strongest predictors of health. Individuals with lower socioeconomic status (SES) are more likely to experience chronic illness, reduced life expectancy, and limited access to health resources (PHAC, 2024).
Employment and Working Conditions. Stable employment contributes to financial security and mental well-being. Conversely, unemployment, unsafe work environments, and job dissatisfaction increase stress and negatively affect health outcomes (Thompson V.D, 2024).
Education. Higher education levels are associated with improved health literacy, better employment opportunities, and increased ability to access medical care. Education empowers individuals to make informed health decisions (Government of Canada, 2024).
Childhood Experiences. Early childhood development has long-term effects on physical, emotional, and cognitive health. Adverse childhood experiences may increase vulnerability to chronic disease later in life (PHAC, 2024).
Physical Environment. The natural and built environments—including housing quality, air and water safety, and workplace conditions—directly influence health status.
Social Support and Coping Skills. Strong social networks and community connections enhance mental and physical health. Social environments are shaped by relationships, culture, and living conditions (PHAC, 2024).
Healthy Behaviours. Lifestyle choices such as smoking, poor diet, and physical inactivity significantly affect morbidity and mortality rates.
Access to Health Services. Availability of primary care, health promotion, and disease prevention services improves overall population health. (Government of Canada, 2024).
Biology and Genetic Endowment. Genetic factors may predispose individuals to certain diseases, though these risks often interact with social and environmental influences.
Gender, Sex, and Sexuality. Biological differences and social identities influence health risks, mental health outcomes, and access to services (PHAC, 2024).
Culture. Cultural beliefs and values shape health behaviours, perceptions of illness, and willingness to seek treatment.
Race and Racism. Despite protections under the Canadian Human Rights Act, systemic racism continues to contribute to disparities in health outcomes and access to care (Government of Canada, 2024).
The Population Health Approach
To address these determinants, PHAC promotes a population health approach that focuses on improving the health of entire populations rather than solely treating illness (PHAC, 2024). This approach includes eight key elements: focusing on measurable health indicators; addressing determinants and their interactions; using evidence-informed decision-making; investing in upstream prevention; applying multiple intervention strategies; collaborating across sectors; engaging the public; and demonstrating accountability for outcomes.
The social determinants of health highlight the importance of addressing conditions beyond clinical care to improve overall well-being. Canada’s population health approach provides a framework for reducing inequities through prevention, collaboration, and evidence-informed policy. Understanding these determinants is essential to creating a more equitable and effective health care system.
References
Government of Canada. (2024). Social determinants of health and health inequalities. https://www.canada.ca/en/public-health/services/health-promotion/population-health/what-determines-health.html
Public Health Agency of Canada. (2024) Public Health Agency of Canada 2023–24 Departmental Plan – Canada.ca
Thompson, V.D. (2024). Health and health care delivery in Canada (4th ed.). Elsevier.
A Multi-Level Approach to Advancing Indigenous Health Equity in Canada – February 24th 2026
Health inequities experienced by Indigenous, Inuit, and Métis peoples in Canada cannot be explained by individual behaviours or isolated gaps in service deliveries. There is substantial evidence to demonstrate these disparities are structurally produced through the ongoing effects of broad colonialism, systemic racism, and inequitable conditions. Advancing Indigenous health equity requires a coordinated, multi-level approach that addresses structural determinants, health system reform, community capacity, and the broader social and environmental conditions shaping daily life.
Greenwood, Atkinson, and Sutherland (2017) conceptualize colonialism as a structural determinant of health that continues to shape the living conditions of Indigenous, Inuit, and Métis peoples. Colonial policies dismantled Indigenous governance systems, displaced communities from land-based economies, imposed residential schooling, and created fragmented jurisdictional responsibility for health and social services. These processes have contributed to inequities in income, housing, education, food security, and access to culturally appropriate care.
Health inequities are avoidable and unjust because they are embedded in policy and institutional arrangements (Greenwood et al., 2017). Meaningful progress requires systemic change including Indigenous self-determination in health governance and sustained structural reform rather than incremental programmatic responses. Recent national data reinforce the persistence of systemic barriers within the Canadian health system. Statistics Canada (2024) reports that 30% of Métis, 29% of Inuit and 32% of Indigenous people living off reserve experience unmet health care needs within the past year. Gaps were particularly evident in mental health care. While 47% of First Nations people living off reserve, 43% of Métis, and 35% of Inuit reported needing mental health services, only a minority indicated that their needs were fully met (Statistics Canada, 2024).
Geographic barriers further intensify inequities, with approximately 40% of Inuit participants reported the need to travel outside their community to access care (Statistics Canada, 2024). Experiences of racism remain a prevalent issue with roughly one in five Indigenous adults reporting discrimination from health care providers (Statistics Canada, 2024). These findings reveal ongoing institutional shortcomings that undermine trust and restrict access to care.
A strong majority of Indigenous participants indicated that access to traditional medicines and culturally grounded healing practices as important to their well-being (Statistics Canada, 2024), highlighting a misalignment between Indigenous health priorities and mainstream service delivery models.
Health inequities must also be understood within the context of broader social and environmental determinants. Marcone, Madan, and Grodzinski (2020) demonstrate that eating behaviours in Canada are shaped by sociological and environmental influences, including income, education, food availability, infrastructure, and marketing practices. These factors constrain individual choice and structure dietary patterns. For many Indigenous communities, food insecurity is compounded by geographic isolation, high transportation costs, and the erosion of traditional food systems linked to land dispossession. Nutrition-related health outcomes must therefore be situated within colonial and environmental contexts rather than framed as individual lifestyle issues (Greenwood et al., 2017; Marcone et al., 2020).
The expansion of Indigenous-led health care models represents a key pathway toward health equity. The Canadian Medical Association (2026) describes Indigenous-led health care as grounded in community governance, Indigenous knowledge systems, and the integration of traditional healing practices alongside Western medicine. These models emphasize holistic understandings of health encompassing spiritual, emotional, physical, and relational dimensions.
Indigenous-led approaches incorporate land-based healing, maternal and family-centered services, food independence initiatives, and trauma-informed care. Beyond service adaptation, these models represent structural reform by repositioning authority, knowledge, and decision-making within Indigenous communities. Such approaches align directly with Greenwood et al.’s (2017) assertion that Indigenous self-determination is foundational to achieving health equity.
Advancing Indigenous health equity requires coordinated actions across multiple levels. At the structural level, policy reform must address jurisdictional fragmentation, funding inequities, and systemic racism. At the health system level, institutions must embed cultural safety and integrate Indigenous knowledge systems. At the community level, land-based initiatives, food sovereignty programs, and community-controlled services should be supported. At the individual level, health behaviours must be understood as shaped by broader structural and environmental conditions.
In conclusion, the research and national data demonstrate that Indigenous health inequities in Canada are structurally produced and systemically reinforced. High rates of unmet care, geographic barriers, and discrimination reflect institutional failures rather than individual shortcomings. At the same time, strong support for indigenous-led and culturally grounded services point to viable and evidence-based pathways forward.
Advancing health equity requires structural reform, institutional accountability, community leadership, and Indigenous self-determination. A multi-level approach provides a comprehensive framework for transforming health systems to achieve equitable outcomes.
References
Canadian Medical Association. (2026). What is Indigenous-led health care in Canada? CMA Healthcare for Real. https://www.cma.ca/healthcare-for-real/what-indigenous-led-health-care-canada
Greenwood, M., Atkinson, D., & Sutherland, J. (2017). Supporting health equity for First Nations, Inuit and Métis peoples. Healthcare Policy, 12(2), 31–36.
Marcone, M. F., Madan, P., & Grodzinski, B. (2020). An overview of the sociological and environmental factors influencing eating food behavior in Canada. Frontiers in Nutrition, 7, Article 77. https://doi.org/10.3389/fnut.2020.00077
Statistics Canada. (2024, November 4). Health care access and experiences among Indigenous people, 2024. https://www150.statcan.gc.ca/n1/daily-quotidien/241104/dq241104a-eng.htm
Healing Beyond the System: A Multilevel Approach to Indigenous Health Equity in Canada – March 10th 2026
Health inequities experienced by Indigenous, Inuit, and Métis peoples in Canada cannot be explained solely by individual behaviours or gaps in health services. Instead, these disparities are shaped by historical and structural forces that influence living conditions, access to care, and overall well-being. Research demonstrates that colonialism, systemic racism, and inequitable social conditions continue to shape Indigenous health outcomes today. Addressing these inequities requires a multilevel approach to health, which recognizes that health is influenced by interconnected structural, institutional, community, and individual determinants.
A multilevel model of health which is often described as the socio-ecological modelrecognizes that health outcomes are influenced by factors operating at several levels of society. These include public policy, health systems, community environments, and individual behaviours. Rather than focusing only on personal lifestyle choices, this framework emphasizes how broader social, political, and environmental contexts shape opportunities for health. Applying a multilevel perspective is particularly important when examining Indigenous health inequities in Canada, where colonial systems have profoundly influenced social conditions and health care access.
Colonialism as a Structural Determinant of Health
Colonialism is widely recognized as a structural determinant of Indigenous health. Greenwood, Atkinson, and Sutherland (2017) describe colonialism as a system that historically reshaped the social, political, and economic conditions of First Nations, Inuit, and Métis peoples. Colonial policies dismantled Indigenous governance systems, displaced communities from traditional lands and land-based economies, and imposed institutions such as residential schools. These policies disrupted cultural continuity and created long-term social and economic inequities.
Colonial systems also established fragmented jurisdictional responsibility for Indigenous health services between federal and provincial governments. This fragmentation has contributed to gaps in service delivery and inconsistent access to health care. Over time, these policies have contributed to disparities in housing, education, food security, employment, and access to culturally appropriate care (Greenwood et al., 2017).
Scholars increasingly describe colonialism as a distal determinant of health, meaning it shapes the broader political and economic environments that influence health outcomes across generations (Czyzewski, 2011). These structural forces influence intermediate determinants such as infrastructure, income, and access to services, which ultimately affect individual health outcomes. Because these inequities arise from policy decisions and institutional arrangements, they are considered avoidable and unjust.
Barriers to Health Care Access
In 2024, Statistics Canada reported evidence showing that systemic barriers in health care continue to be widespread for Indigenous peoples in Canada. Mental health care gaps were particularly significant, with many individuals reporting their need were not adequately met. These findings reveal persistent limitations within the Canadian health system in meeting the needs of Indigenous populations.
| Statistics Canada (2024) | Indigenous People | Métis | Inuit |
| Off-reserve experience unmet health care | 32% | 30% | 29% |
| Mental health care needs were not met | 47% | 43% | 35% |
Table 1: Statistics Canada Reports from 2024, from individuals who voluntarily reported.
Geographic barriers also further intensify inequities as approximately 40% of Inuit participants required travel outside their communities to access healthcare services, demonstrating limitation in northern and remote regions (Statistics Canada, 2024). Experiences of racism and discrimination continued to restrict access to care. Approximately one in five Indigenous adults reported discrimination from health care providers (Statistics Canada, 2024). Collectively these findings reveal that Indigenous health inequities are not isolated events but are embedded within a broader system of structural violence linked to colonial policies and institutional racism. These experiences contribute to chronic disease prevalence, life expectancy, and access to culturally appropriate care.
Research shows that these inequities are embedded within broader systems of structural violence linked to colonial policies and institutional racism (Browne et al., 2016). These systemic conditions contribute to disparities in life expectancy, chronic disease prevalence, and access to appropriate health services.
Social and Environmental Determinants of Health
Health inequities must also be understood within the broader context of social and environmental determinants. Marcone, Madan, and Grodzinski (2020) demonstrate that health behaviours, including dietary patterns, are shaped by social and environmental influences such as income, education, infrastructure, food availability, and marketing practices. These factors limit the extent to which individuals can freely choose healthy behaviours.
For many Indigenous communities, food insecurity is intensified by geographic isolation and high transportation costs. Nutritious food in northern communities is often significantly more expensive than in southern urban centres. Limited infrastructure and access to grocery stores further constrain healthy food choices.
Colonial land dispossession has also disrupted traditional food systems that historically supported Indigenous health and cultural practices. Restrictions on land access and traditional harvesting activities have weakened Indigenous food sovereignty and contributed to increased reliance on market food systems.
These realities demonstrate that nutrition-related health outcomes cannot be understood solely as individual lifestyle choices. Instead, they must be examined within broader historical, political, and environmental contexts (Greenwood et al., 2017; Marcone et al., 2020).
Indigenous-Led Health Care Models
Indigenous-led health care models represent a promising pathway toward improving health equity. Indigenous-led systems are grounded in community governance, Indigenous knowledge systems, and culturally appropriate approaches to care (Canadian Medical Association, 2026).

These models emphasize holistic understandings of health that include physical, emotional, spiritual, and relational dimensions. Rather than focusing solely on disease treatment, Indigenous health frameworks prioritize balance, connection to land, and community well-being.
Indigenous-led initiatives often incorporate land-based healing programs, culturally grounded mental health services, maternal and family-centered care, trauma-informed approaches, and food sovereignty initiatives. These programs integrate traditional healing practices alongside Western medical care.
Importantly, Indigenous-led models represent more than adaptations to existing services. They reflect structural transformation by repositioning authority and decision-making within Indigenous communities. Research demonstrates that strengthening Indigenous governance over health services is essential for improving health outcomes and advancing equity (Lavoie et al., 2021).
Applying a Multilevel Model to Indigenous Health
A multilevel framework helps illustrate how coordinated actions across different levels can address health inequities. At the structural level, policy reforms must address systemic inequities such as jurisdictional fragmentation, funding disparities, and systemic racism within institutions. Investments in housing, education, food systems, and infrastructure are also critical determinants of health. At the health system level, institutions must implement culturally safe practices, integrate Indigenous knowledge systems, and increase Indigenous representation within health professions. Institutional accountability is also necessary to address discrimination and ensure equitable care. Research indicates that Indigenous patients frequently experience complex health challenges shaped by social determinants, cultural contexts, and systemic barriers within health systems (Sehgal et al., 2024). At the community level, community-driven initiatives such as land-based healing programs, food sovereignty initiatives, and community-controlled health services strengthen cultural continuity and local capacity.
Finally, at the individual level, health behaviours such as diet, mental health care, and physical activity should be understood within the broader structural and environmental conditions that shape available choices. Addressing inequities at only one level is unlikely to produce meaningful change. Instead, coordinated action across all levels is necessary to improve health outcomes.
Moving Toward Health Equity
Evidence clearly shows that Indigenous health inequities in Canada are structurally produced and systemically reinforced. High rates of unmet care needs, geographic barriers, and experiences of discrimination reflect institutional shortcomings rather than individual failings.
At the same time, strong support for Indigenous-led and culturally grounded health services highlights promising pathways forward. Indigenous governance, culturally appropriate care, and community-based health initiatives offer evidence-based strategies for improving health outcomes.
Advancing Indigenous health equity requires structural reform, institutional accountability, community leadership, and Indigenous self-determination. A multilevel approach provides a comprehensive framework for addressing the root causes of inequities and transforming health systems. By recognizing the interconnected relationships between policy, environment, institutions, and community well-being, Canada can move closer to building a health system that supports equitable outcomes for Indigenous, Inuit, and Métis peoples.
References
Browne, A. J., Varcoe, C., Lavoie, J., Smye, V., Wong, S., Krause, M., et al. (2016). Enhancing health care equity with Indigenous populations: Evidence-based strategies from an ethnographic study. BMC Health Services Research, 16, 544.
Canadian Medical Association. (2026). What is Indigenous-led health care in Canada? https://www.cma.ca/healthcare-for-real/what-indigenous-led-health-care-canada
Congress of Aboriginal Peoples. (n.d.). Indigenous determinants of health. Enviromental-Fact-Sheet-Final.pdf
Czyzewski, K. (2011). Colonialism as a broader social determinant of health. International Indigenous Policy Journal, 2(1).
Fitzpatrick, Kayla et al. Understanding Indigenous peoples experiences to inform recommendations for improving cultural safety and care in radiation therapy centres in Alberta, Canada. Journal of Medical Imaging and Radiation Sciences, Volume 55, Issue 3, 101722
Greenwood, M., Atkinson, D., & Sutherland, J. (2017). Supporting health equity for First Nations, Inuit and Métis peoples. Healthcare Policy, 12(2), 31–36.
Lavoie, J. G., Kinew, K. A., & Katz, A. (2021). Decolonizing health in Canada: A Manitoba First Nation perspective. International Journal for Equity in Health, 20, 1–12.
Marcone, M. F., Madan, P., & Grodzinski, B. (2020). An overview of the sociological and environmental factors influencing eating food behavior in Canada. Frontiers in Nutrition, 7, 77.
Sehgal, A., Henderson, R., Murry, A., Crowshoe, L., & Barnabe, C. (2024). Advancing health equity for Indigenous peoples in Canada. BMC Primary Care, 25, 144.
Statistics Canada. (2024). Health care access and experiences among Indigenous people, 2024. The Daily — Health care access and experiences among Indigenous people, 2024
